

Key Takeaways For many years, clinical trials have been misunderstood by patients and families. A common myth is that clinical trials are only considered when all other treatments have failed. In reality, this is far from the truth. Today, clinical trials for cancer patients are an essential part of modern medicine and are often available alongside standard treatments. These trials test new drugs, therapies, and treatment strategies that may offer improved outcomes, fewer side effects, or more personalised care. Doctors and researchers across the world rely on cancer research clinical trials to discover safer and more effective cancer treatments. Many of the therapies used in hospitals today, such as immunotherapy, targeted therapy, and advanced radiation treatments, became available only because patients participated in clinical trials. What Are Clinical Trials in Cancer Care? Clinical trials are carefully designed medical studies that evaluate new approaches to prevent, diagnose, or treat diseases. In oncology, cancer treatment clinical trials test new therapies, combinations of treatments, or innovative treatment technologies. These trials help researchers determine whether a treatment is safe and effective before it becomes widely available. Patients participating in clinical trials for cancer patients receive close monitoring by specialised medical teams, ensuring their safety throughout the study. Importantly, clinical trials follow strict ethical and regulatory guidelines. They are reviewed by scientific committees, regulatory authorities, and ethics boards to protect participants. According to the National Cancer Institute, nearly20% of cancer treatments used today were developed through clinical trials in the last decade. Why Clinical Trials Are Not a “Last Resort” One of the biggest misconceptions about clinical trials for cancer patients is that they are only offered when conventional treatments no longer work. However, many trials are designed for patients at different stages of cancer, including newly diagnosed cases. In some situations, cancer treatment clinical trials may provide access to innovative therapies that are not yet widely available. Participating in clinical trials can offer several advantages: The growing success of cancer research clinical trials is transforming how cancer care evolves worldwide. Understanding Cancer Clinical Trial Phases Every new treatment must pass through several stages before it becomes approved for public use. These stages are known as cancer clinical trial phases. Understanding the cancer clinical trial phases helps patients and families know what to expect. Phase 1 Trials Phase 1 trials are the first step in testing a new drug in humans. These trials focus on safety, dosage, and identifying potential side effects. Phase 2 Trials In Phase 2 trials, researchers study how well the treatment works against a specific type of cancer. Phase 3 Trials Phase 3 trials compare the new treatment with the current standard treatment to determine which is more effective. Phase 4 Trials After a drug is approved, Phase 4 trials continue monitoring long-term safety and effectiveness. These structured cancer clinical trial phases ensure that every treatment undergoes rigorous testing before becoming part of routine care. Benefits of Clinical Trials in Cancer Treatment There are several important benefits of clinical trials in cancer that patients should understand. Access to Innovative Therapies Patients may gain access to treatments that are not yet widely available but show promising results. Advanced Monitoring Participants receive careful monitoring from specialised oncology teams throughout the study. Personalised Treatment Approaches Some trials focus on precision medicine, tailoring treatments based on genetic markers or tumour characteristics. Contribution to Medical Progress Patients who participate in cancer research clinical trials help scientists develop better therapies for future generations. These benefits of clinical trials in cancer make them an important option to consider during treatment planning. Cancer Clinical Trials Statistics Understanding cancer clinical trials statistics helps highlight the impact these studies have on medical progress. Research shows that clinical trials have contributed significantly to improving cancer survival rates over the past several decades. According to the American Cancer Society, the overall 5-year survival rate for cancer in the United States has increased from about 49% in the 1970s to nearly 69% today, largely due to advances developed through clinical trials. Global participation in cancer research clinical trials continues to grow as researchers search for more effective therapies. However, participation rates remain relatively low. Studies suggest that less than 5% of adult cancer patients participate in clinical trials, highlighting the need for greater awareness. These cancer clinical trials statistics emphasise how important patient participation is for medical innovation. Cancer Vaccine Clinical Trials: A New Frontier One exciting area of research involves the development of cancer vaccines. A cancer vaccine clinical trial investigates vaccines designed to stimulate the immune system to recognise and attack cancer cells. Unlike traditional vaccines that prevent infections, cancer vaccines may help treat existing cancers by strengthening the body’s immune response. Several promising cancer vaccine clinical trial programs are currently exploring treatments for cancers such as: Advances in immunotherapy and mRNA technology are accelerating research in this field. According to research published in the journal Nature Reviews Cancer, therapeutic cancer vaccines are being studied in hundreds of ongoing clinical trials worldwide. Clinical Trials in India for Cancer India is becoming an increasingly important hub for oncology research. Today, many global pharmaceutical companies and research institutions conduct clinical trials in India for cancer to evaluate new therapies in diverse populations. The growth of clinical trials in India for cancer offers several benefits: Major cancer centres across the country now participate in cancer research clinical trials. The Clinical Trials Registry of India (CTRI) tracks thousands of ongoing studies, including many cancer treatment clinical trials. Choosing the Best Cancer Clinical Trials When considering participation, patients often ask how to identify the best cancer clinical trials. Choosing the best cancer clinical trials involves several factors: Doctors and oncologists play an important role in guiding patients toward suitable clinical trials for cancer patients based on their specific condition. Patients should always discuss clinical trial options with their oncology team before making a decision. Interpreting Cancer Clinical Trial Results Once a study is completed, researchers analyse and publish the cancer clinical trial results. These cancer clinical
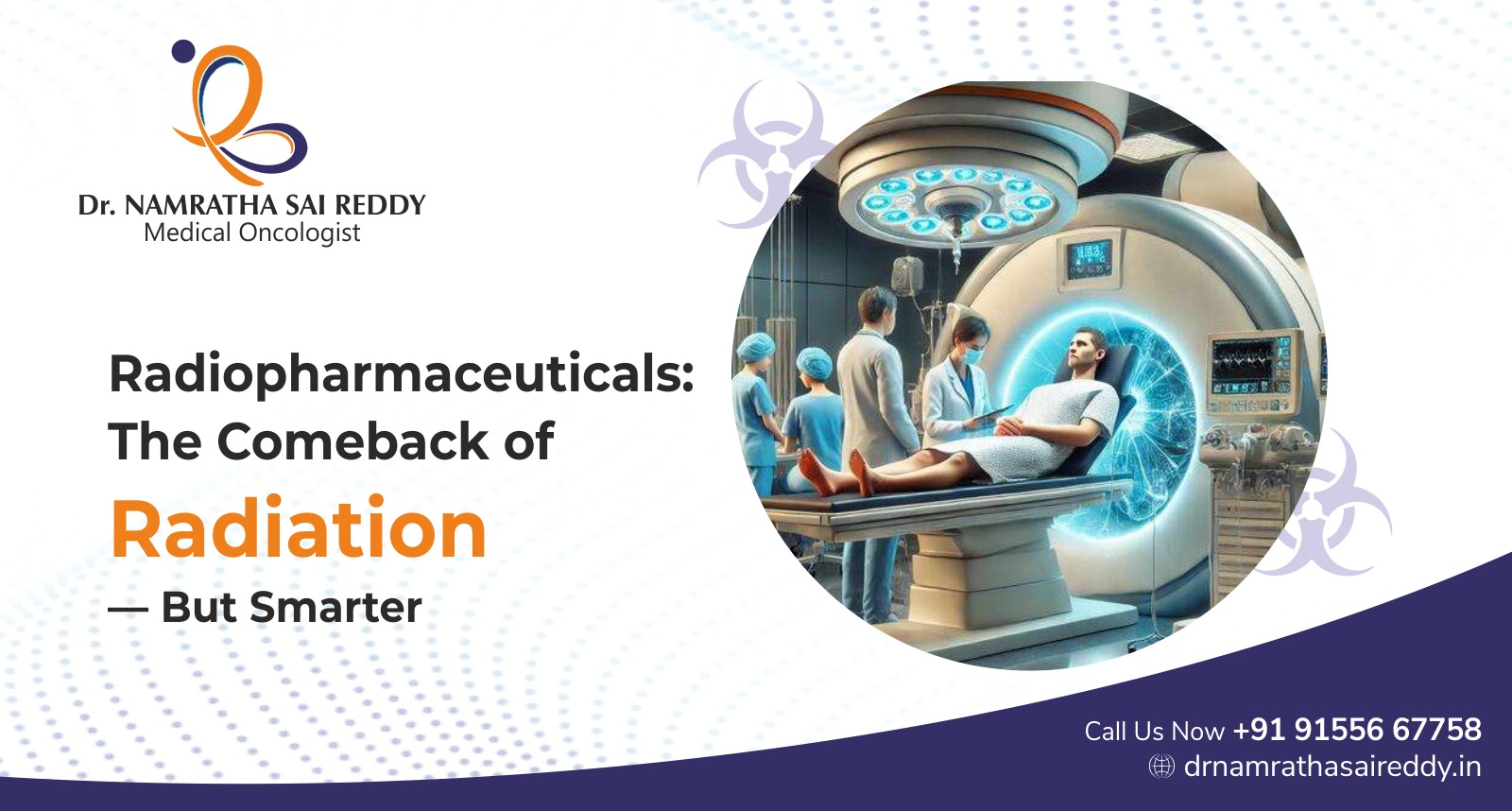
Radiopharmaceuticals: The Comeback of Radiation – But Smarter
Key Takeaways Radiation therapy has been used in cancer treatment for more than a century. Traditionally, radiation has been delivered externally through machines that target tumours from outside the body. While this approach has saved millions of lives, it can sometimes affect surrounding healthy tissues. In recent years, a new wave of targeted nuclear medicine has transformed how radiation is used in oncology. One of the most promising developments is the use of radiopharmaceuticals, specialised radioactive drugs designed to seek out cancer cells and deliver radiation directly to them. As cancer care moves toward precision medicine, radiopharmaceuticals are becoming an important tool in the fight against complex and advanced cancers. What Are Radiopharmaceuticals? To understand nuclear medicine therapies, it is important to ask: what are radiopharmaceuticals? Radiopharmaceuticals are medicinal compounds that contain radioactive isotopes combined with biologically active molecules. These molecules guide the radioactive component to a specific organ, tissue, or tumour in the body. In simple terms, what are radiopharmaceuticals used for? They serve two main purposes: • Diagnosis – helping doctors visualise organs and detect disease through imaging• Treatment – delivering targeted radiation to destroy abnormal cells The radioactive element emits radiation that can either produce images inside the body or damage cancer cells. These drugs are widely used in nuclear medicine procedures such as: According to the International Atomic Energy Agency (IAEA), nuclear medicine procedures using radiopharmaceuticals are performed over 40 million times annually worldwide. Why Radiopharmaceuticals Are Revolutionising Cancer Treatment Traditional radiation therapy typically directs radiation beams from outside the body toward tumours. Although effective, this method may expose nearby healthy tissues to radiation. Modern radiopharmaceuticals take a different approach. They travel through the bloodstream and bind specifically to cancer cells or tumour receptors. This targeted approach offers several advantages: This type of therapy is often called targeted radionuclide therapy or theranostics, a combination of therapy and diagnostics. Recent research shows significant promise for radiopharmaceutical therapies in treating advanced cancers such as prostate cancer and neuroendocrine tumours. A landmark study published in the New England Journal of Medicine showed that Lutetium-177 therapy significantly improved progression-free survival in patients with advanced neuroendocrine tumours. Classification of Radiopharmaceuticals Understanding the classification of radiopharmaceuticals helps explain how they are used in different medical situations. The classification of radiopharmaceuticals generally includes two major groups. 1. Diagnostic Radiopharmaceuticals These are used to detect disease and evaluate organ function. Diagnostic agents emit radiation that can be detected by imaging devices such as PET or SPECT scanners. These scans help doctors identify tumours, detect metastasis, and assess treatment response. Examples include: 2. Therapeutic Radiopharmaceuticals These deliver radiation directly to diseased tissues to destroy cancer cells. Therapeutic agents emit radiation strong enough to damage tumour DNA and inhibit cancer growth. Examples include: This classification of radiopharmaceuticals allows physicians to select the most appropriate compound depending on whether the goal is diagnosis or treatment. Commonly Used Radiopharmaceuticals in Oncology Several commonly used radiopharmaceuticals have become essential tools in modern cancer care. Some widely used examples include: Iodine-131 Used for the treatment of thyroid cancer and hyperthyroidism. Lutetium-177 DOTATATE Used for neuroendocrine tumours that express somatostatin receptors. Radium-223 Dichloride Used for prostate cancer that has spread to the bones. Fluorine-18 FDG Used in PET scans to detect cancer activity in the body. These commonly used radiopharmaceuticals play a critical role in both cancer diagnosis and targeted treatment. According to the National Cancer Institute, PET scans using FDG help doctors detect cancer earlier and evaluate treatment response more accurately. Application of Radiopharmaceuticals in Modern Medicine The application of radiopharmaceuticals is not limited to oncology. These drugs are widely used in several areas of medicine. Oncology Cancer diagnosis and treatment are the most well-known applications of radiopharmaceuticals. Radiotracers help detect tumours, monitor treatment response, and deliver targeted radiation therapy. Cardiology Radiopharmaceutical imaging helps assess heart function and blood flow. Cardiac nuclear imaging is commonly used to diagnose coronary artery disease and evaluate myocardial viability. Neurology Brain imaging using nuclear tracers helps diagnose neurological disorders such as: Endocrinology Radiopharmaceuticals are widely used for thyroid disease diagnosis and treatment. Because of their versatility, the application of radiopharmaceuticals continues to expand across multiple medical specialities. Advantages of Radiopharmaceuticals There are several important advantages of radiopharmaceuticals that make them valuable in modern healthcare. Some key advantages of radiopharmaceuticals include: Targeted Therapy Radiation is delivered directly to tumour cells, reducing exposure to healthy tissues. Precision Medicine Therapies can be tailored based on the molecular characteristics of each patient’s tumour. Early Disease Detection Diagnostic radiopharmaceuticals allow doctors to detect disease at very early stages. Combined Diagnosis and Treatment The concept of theranostics allows doctors to use the same molecular target for both imaging and therapy. Improved Outcomes in Certain Cancers Radiopharmaceutical therapy has shown improved survival outcomes in specific cancer types. According to market research by Grand View Research, the global radiopharmaceutical market is expected to grow significantly due to increasing cancer incidence and advancements in nuclear medicine. Cancer Biotherapy and Radiopharmaceuticals One of the most exciting research areas in oncology is the combination of cancer biotherapy and radiopharmaceuticals. Biotherapy uses biological agents such as antibodies, immune cells, or cytokines to stimulate the immune system to fight cancer. When combined with targeted radiation therapy, cancer biotherapy and radiopharmaceuticals may work synergistically to improve treatment outcomes. For example: Scientific journals such as Cancer Biotherapy and Radiopharmaceuticals publish research on these emerging therapies. The cancer biotherapy and radiopharmaceuticals impact factor reflects the growing interest in this area of cancer research. Storage of Radiopharmaceuticals Because these drugs contain radioactive materials, proper storage of radiopharmaceuticals is extremely important. Hospitals follow strict regulatory guidelines to ensure safety and effectiveness. The storage of radiopharmaceuticals typically requires: Radiopharmaceuticals often have short half-lives, which means they must be used within a limited time after preparation. Specialised hospital pharmacies and nuclear medicine units handle the safe preparation and storage of these drugs. Disposal of Radiopharmaceuticals Another critical aspect of nuclear medicine safety is the disposal of radiopharmaceuticals. Since these substances contain radioactive isotopes,

Understanding Chemotherapy Side Effects and How to Manage Them
Chemotherapy remains one of the most widely used treatments for cancer. It works by destroying rapidly dividing cancer cells and preventing them from growing and spreading. While chemotherapy can be highly effective in controlling cancer, it may also affect healthy cells that divide quickly, leading to chemotherapy side effects. Understanding what are the side effects of chemotherapy and learning how to manage them can help patients cope better during treatment. With proper medical care and supportive therapies, many cancer chemotherapy side effects can be controlled or reduced. Key Takeaways What Are the Side Effects of Chemotherapy? Chemotherapy side effects occur because chemotherapy drugs attack rapidly dividing cells in the body, including both cancer cells and some healthy cells. When healthy cells in areas such as the bone marrow, digestive tract, and hair follicles are affected, patients may experience various symptoms during treatment. To answer what are the side effects of chemotherapy, the effects can range from mild discomfort to more noticeable physical changes, depending on the type of drug used and the patient’s overall health. These chemotherapy treatment side effects vary from person to person. Some patients may experience only mild symptoms, while others may experience several common side effects of chemotherapy during treatment cycles. Most symptoms are temporary and improve after treatment ends. Research from the U.S. National Cancer Institute notes that chemotherapy affects healthy cells but many of these cells recover after treatment is completed. Why Do Chemotherapy Side Effects Occur? Chemotherapy side effects occur because chemotherapy drugs cannot always distinguish between cancer cells and healthy cells that divide quickly. As a result, some normal tissues are temporarily affected during treatment. These cancer chemotherapy side effects commonly occur in tissues with rapid cell turnover, including hair follicles, digestive tract lining, and bone marrow. Cells most affected by chemotherapy include: Damage to these cells leads to many common side effects of chemotherapy, such as hair loss, fatigue, anaemia, and digestive discomfort. According to the American Cancer Society, side effects depend on the type of drug, dosage, and length of treatment. What Are the Common Side Effects of Chemotherapy? The common side effects of chemotherapy vary depending on the medications used and the patient’s overall health. While not everyone experiences all symptoms, several side effects occur frequently during chemotherapy treatment. Common chemotherapy side effects include: Understanding what are the side effects of chemotherapy helps patients prepare for treatment and seek timely medical support when symptoms appear. Research suggests that fatigue is among the most frequently reported cancer chemotherapy side effects, affecting up to 80% of patients undergoing chemotherapy. Chemotherapy vs Radiation Side Effects: What Is the Difference? Understanding chemotherapy vs radiation side effects is important because these two cancer treatments affect the body in different ways. Chemotherapy circulates throughout the bloodstream and can affect many parts of the body, while radiation therapy targets a specific area. Key differences in chemotherapy vs radiation side effects Chemotherapy Radiation therapy Because chemotherapy acts throughout the body, cancer chemotherapy side effects may appear more widespread than radiation-related symptoms. What Are the Long-Term Chemotherapy Treatment Side Effects? While most chemotherapy treatment side effects are temporary, some patients may experience long-term or late effects depending on the drugs used and the duration of treatment. Certain chemotherapy drugs can affect organs such as the heart, nerves, or kidneys if used at high doses or over long periods. Possible long-term chemotherapy side effects Although these complications are less common, doctors monitor patients carefully during treatment to detect early signs of long-term cancer chemotherapy side effects. How Can Chemotherapy Side Effects Be Managed? Managing chemotherapy side effects is an essential part of cancer care. Doctors often prescribe supportive medications and recommend lifestyle adjustments to help patients cope with treatment. Many chemotherapy side effects can be reduced with early intervention and supportive care. Ways to manage chemotherapy treatment side effects Supportive care strategies have improved significantly over the years, allowing doctors to manage many common side effects of chemotherapy more effectively. According to the World Health Organization, supportive therapies play an important role in improving the quality of life for cancer patients undergoing treatment. When Should Patients Report Chemotherapy Side Effects to Their Doctor? Patients should inform their doctor whenever chemotherapy side effects become severe, persistent, or interfere with daily activities. Early medical attention can help prevent complications and improve comfort during treatment. Some symptoms require immediate medical attention, especially if they indicate infection or severe reactions. Symptoms that should be reported immediately Prompt reporting helps doctors adjust treatment plans and manage chemotherapy ke side effect symptoms safely. Living Well During Chemotherapy Understanding what are the side effects of chemotherapy allows patients to prepare mentally and physically for treatment. While chemotherapy treatment side effects can be challenging, modern supportive care has made it possible for many patients to continue daily activities during treatment. Advances in cancer medicine are also improving the management of cancer chemotherapy side effects, helping patients maintain a better quality of life throughout their cancer journey. With proper medical guidance, nutrition, emotional support, and symptom management, many patients successfully navigate chemotherapy while continuing their path toward recovery. FAQs 1. What are the side effects of chemotherapy? Chemotherapy side effects may include fatigue, nausea, hair loss, mouth sores, and increased risk of infections. 2. Why do chemotherapy side effects occur? Cancer chemotherapy side effects occur because chemotherapy drugs affect both cancer cells and rapidly dividing healthy cells. 3. What are the most common side effects of chemotherapy? The common side effects of chemotherapy include fatigue, nausea, hair loss, and lowered immunity. 4. Are chemotherapy side effects permanent? Most chemotherapy treatment side effects are temporary and improve after treatment ends. 5. What is the difference between chemotherapy vs radiation side effects? In chemotherapy vs radiation side effects, chemotherapy affects the entire body while radiation side effects occur mainly in the treated area. 6. Can chemotherapy side effects be prevented? While not all chemotherapy ke side effects can be prevented, many can be reduced with supportive medications. 7. How
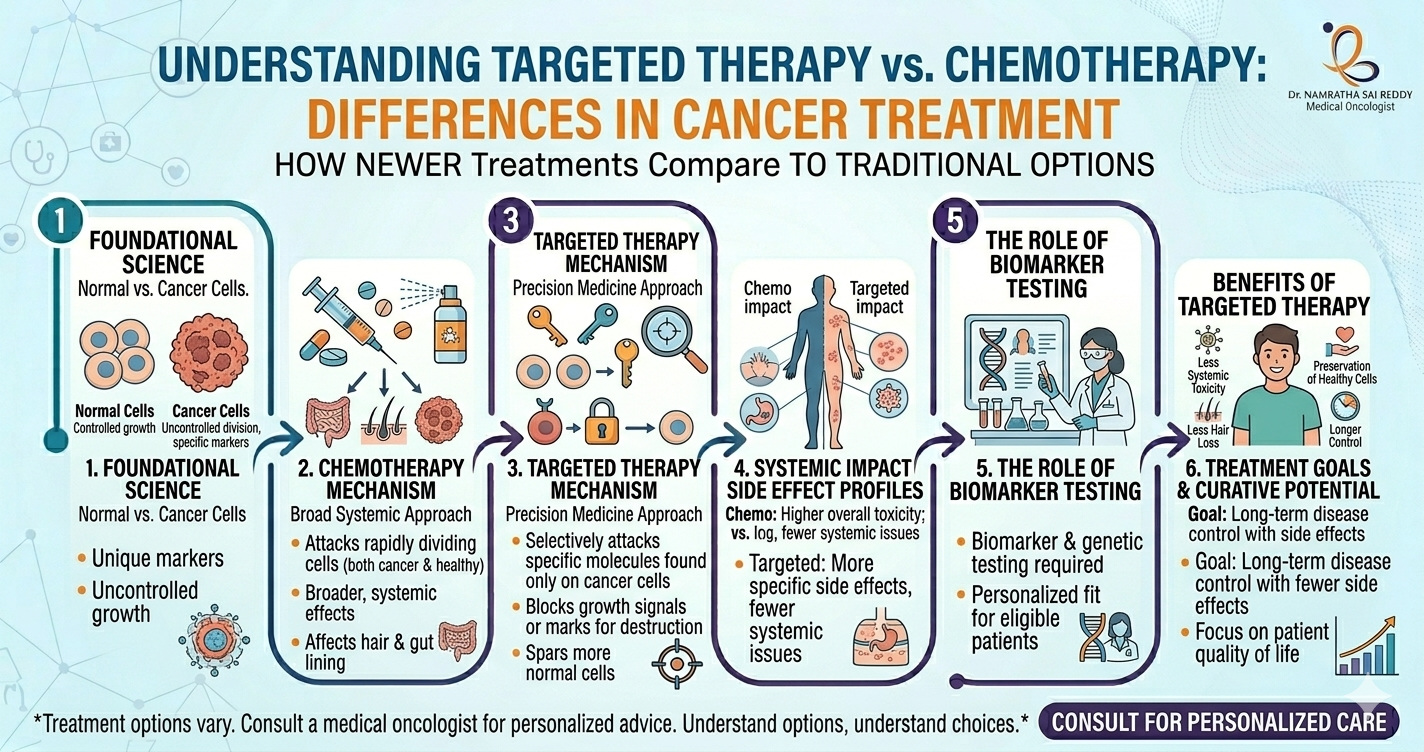
Understanding Targeted Therapy in Cancer Treatment: How It Differs from Chemotherapy
Cancer treatment is rapidly evolving with the development of precision medicine. Traditional treatments, such as chemotherapy, attack rapidly dividing cells across the body, but newer approaches focus on the biological mechanisms that drive cancer growth. One of the most important advances in modern oncology is targeted therapy, which allows doctors to treat cancer by attacking specific genetic mutations or proteins in cancer cells. Understanding what is targeted therapy in cancer, how it works, and how targeted therapy vs chemotherapy differs from chemotherapy can help patients better understand modern cancer treatment options. Key Takeaways What Is Targeted Therapy in Cancer? Targeted therapy is a type of cancer treatment that uses drugs designed to attack specific molecular targets involved in cancer growth and survival. To understand what is targeted therapy in cancer, it is important to know that many cancers develop due to genetic mutations that activate abnormal proteins or signalling pathways. Unlike traditional chemotherapy, targeted therapy for cancer focuses on the biological mechanisms that allow cancer cells to grow, divide, and spread. These therapies may block proteins that signal cancer cells to grow, interfere with blood vessel formation that feeds tumours, or trigger cancer cell death. Advances in genomic testing have helped identify many actionable targets, enabling doctors to design personalised treatment strategies based on the molecular profile of each tumour. How Does Targeted Therapy Work? Targeted therapy works by interfering with specific molecules or pathways that cancer cells depend on for survival. These targets may include proteins on the cell surface, enzymes inside the cell, or genetic mutations that drive uncontrolled growth. Once these targets are identified, targeted therapy for cancer uses drugs designed to block them and stop cancer progression. Key ways targeted therapy works: Research shows that patients receiving matched targeted therapies often experience improved overall survival and progression-free survival compared with patients who do not receive targeted treatments. Targeted Therapy vs Chemotherapy: What Is the Difference? The difference between targeted therapy vs chemotherapy lies mainly in precision and mechanism of action. Chemotherapy works by destroying rapidly dividing cells throughout the body, which includes cancer cells but also healthy cells such as hair follicles and cells in the digestive tract. In contrast, targeted therapy vs chemotherapy involves drugs designed to attack specific molecular abnormalities found in cancer cells. Key differences in targeted therapy vs chemotherapy Chemotherapy Targeted therapy Studies in patients with metastatic renal cell carcinoma have shown that targeted treatments improved survival rates compared with non-targeted therapies, with higher survival percentages at 1-, 2-, and 3-year follow-ups. Targeted Therapy vs Immunotherapy: How Are They Different? The difference between targeted therapy vs immunotherapy lies in how the treatments fight cancer. Targeted therapy directly blocks molecules that cancer cells need to grow, while immunotherapy works by stimulating the immune system to recognise and destroy cancer cells. Both therapies are considered forms of precision medicine, but they operate through different biological mechanisms. Understanding targeted therapy vs immunotherapy Targeted therapy Immunotherapy Research suggests that combining targeted therapy with immunotherapy may further improve survival outcomes in certain cancers, such as liver cancer. What Are the Possible Targeted Therapy Side Effects? Although targeted therapy is designed to be more precise, patients can still experience targeted therapy side effects because some targeted pathways also exist in normal cells. These side effects vary depending on the drug and the biological pathway being targeted. Common targeted therapy side effects Studies evaluating targeted drugs in certain cancers have shown that while side effects may occur more frequently than with a placebo, they are generally manageable with proper monitoring and supportive care. What Is the Targeted Therapy Success Rate? The targeted therapy success rate depends on several factors, including cancer type, genetic mutation, stage of disease, and patient health. In cancers with identifiable molecular drivers, targeted treatments have significantly improved survival outcomes. For example, research in advanced non-small cell lung cancer showed that patients receiving targeted therapy had a median overall survival of about 45 months compared with 17 months for chemotherapy alone, demonstrating a substantial improvement. Factors influencing the targeted therapy success rate These results highlight how targeted therapy for cancer can dramatically improve treatment outcomes when the correct molecular target is identified. When Do Doctors Recommend Targeted Therapy? Doctors recommend targeted therapy for cancer when genetic or biomarker testing reveals specific molecular targets that can be treated with targeted drugs. This approach is an important part of precision oncology. Situations where targeted therapy may be recommended With advances in genomic sequencing and biomarker testing, doctors can increasingly tailor treatment strategies to the individual characteristics of each patient’s cancer. Why Is Targeted Therapy Considered a Breakthrough in Cancer Treatment? Targeted therapy is considered a breakthrough because it shifts cancer treatment from a generalised approach to a personalised one. Instead of broadly destroying cells, the therapy focuses on the molecular drivers responsible for tumour growth. Reasons targeted therapy for cancer is revolutionary With ongoing research and development, new targeted drugs continue to expand treatment possibilities for patients with previously difficult-to-treat cancers. Moving Toward Personalised Cancer Care Understanding what is targeted therapy in cancer, the differences between targeted therapy vs chemotherapy, and the role of targeted therapy vs immunotherapy helps patients better navigate modern cancer care. As research continues to uncover new molecular targets, targeted therapy is expected to play an even larger role in oncology. This approach represents one of the most important steps toward precision medicine—delivering treatments that are tailored to the unique biology of each patient’s cancer. FAQs 1. What is targeted therapy in cancer? Targeted therapy is a cancer treatment that attacks specific genes, proteins, or molecular pathways that allow cancer cells to grow. 2. How is targeted therapy different from chemotherapy? In targeted therapy vs chemotherapy, targeted therapy focuses on specific cancer cell mechanisms, while chemotherapy attacks all rapidly dividing cells. 3. Is targeted therapy used for all cancers? No. Targeted therapy for cancer works best when the tumour contains specific genetic mutations or molecular targets. 4. What are common targeted therapy side effects?
Why Cancer Cases Are Increasing in Younger Adults: What Doctors Are Observing
Cancer has traditionally been considered a disease that primarily affects older adults. However, doctors across the world are increasingly observing a shift in this pattern. More people in their 20s, 30s, and 40s are being diagnosed with cancer compared with previous decades. This emerging trend has raised important questions about lifestyle changes, environmental exposure, and evolving health patterns. In India as well, oncologists and physicians are noticing a gradual rise in cancer cases in India, particularly among younger individuals. While improved detection and awareness play a role, researchers believe several additional factors may be contributing to the increase. According to the World Health Organization, cancer remains one of the leading causes of death globally. Meanwhile, data from the International Agency for Research on Cancer estimates that over 1.4 million new cancer diagnoses occur annually in India, highlighting the growing burden of cancer cases in India. Key Takeaways Are Cancer Diagnoses Increasing in Younger Adults? Doctors worldwide are reporting more cancer diagnoses in people under 50. Research suggests early-onset cancers are rising globally, making awareness and early screening increasingly important for younger populations. Key statistics These findings confirm that cancer cases increasing among younger populations is becoming an important global health concern. Why Are Doctors Seeing More Cancer Cases in Young Adults? Multiple factors, such as lifestyle changes, environmental exposures, obesity, dietary habits, and genetic influences, may contribute to rising cancer diagnoses in younger adults across many countries. There is no single explanation for why cancer cases are increasing in India and globally. Instead, researchers believe several interconnected factors may be contributing to the rise. Lifestyle changes Modern lifestyles have changed dramatically over the past few decades. Possible risk factors include: These lifestyle shifts may affect metabolism, hormones, and inflammation, potentially influencing cancer risk. Environmental exposures Environmental factors are also being studied as possible contributors to the increase in cancer cases. Possible exposures include: Rapid urbanisation and environmental changes may influence long-term health risks. Which Types of Cancer Are Increasing in Younger Adults? Several cancers, including breast, colorectal, thyroid, and stomach cancers, are being diagnosed more frequently in younger adults, suggesting that early-onset cancer trends are affecting multiple organs. Doctors are observing increasing rates of several cancer types in younger populations. Common cancers seen in younger adults Breast cancer One of the most notable trends is the rise in breast cancer cases in India, particularly among women under 45. Some hospital-based studies in India suggest that a significant proportion of breast cancer patients are younger than 50, which is higher than in several Western countries. Colorectal cancer Colorectal cancer is increasingly being diagnosed in people under 50 in many parts of the world. Thyroid cancer Improved detection partly explains rising cases, but real increases may also exist. Gastrointestinal cancers Some studies suggest increases in stomach and pancreatic cancers among younger individuals. These trends highlight why understanding why cancer cases are increasing in India is becoming increasingly important. Is Better Detection Responsible for Rising Cancer Numbers? Improved screening and diagnostic technologies have increased the detection of cancers earlier, but experts believe better detection alone cannot fully explain the rising number of diagnoses. Modern medicine now includes: Because of these improvements, some cancer cases that might previously have gone undetected are now diagnosed earlier. However, researchers believe that detection improvements do not fully explain why cancer cases increasing worldwide. Lifestyle and environmental changes likely play a significant role. Why Is Breast Cancer Increasing in Younger Women? Hormonal changes, lifestyle factors, delayed pregnancies, obesity, and genetic predisposition may contribute to rising breast cancer cases in India, especially among women under the age of 45. Possible contributing factors Hormonal influences Changes in reproductive patterns, such as delayed childbirth, may influence hormonal exposure. Lifestyle changes Risk factors include: Genetic factors Family history and inherited genetic mutations may increase risk in some individuals. Because of these trends, doctors emphasise awareness of breast health and early evaluation of symptoms. What Symptoms Should Younger Adults Watch For? Persistent symptoms such as unexplained weight loss, unusual lumps, prolonged fatigue, or abnormal bleeding should never be ignored and should be evaluated by a doctor promptly. One challenge with rising cancer cases in India is that younger individuals often assume they are too young to develop cancer. However, early medical evaluation is essential. Symptoms that should not be ignored Recognising these warning signs early can lead to timely diagnosis and more effective treatment. How Can Younger Adults Reduce Cancer Risk? Adopting healthy lifestyle habits, maintaining a balanced diet, exercising regularly, avoiding tobacco, limiting alcohol, and undergoing recommended health screenings can help reduce cancer risk. While not all cancers are preventable, several lifestyle changes may help reduce risk. Preventive measures include Public awareness about why cancer cases are increasing in India is essential to encourage healthier lifestyle choices. Take Early Symptoms Seriously and Prioritise Preventive Care The rising number of cancer cases in India and globally highlights the need for greater awareness and proactive health management. As doctors observe cancer cases increasing among younger adults, early detection and preventive strategies are becoming more important than ever. Understanding why cancer cases are increasing in India can help individuals make informed health decisions and encourage early medical consultation when symptoms appear. By maintaining healthy lifestyles, staying aware of warning signs, and seeking timely medical care, individuals can significantly improve their chances of early diagnosis and successful treatment. Frequently Asked Questions (FAQs) 1. Are cancer cases increasing among younger adults? Yes, studies worldwide show a growing number of early-onset cancers in people under 50, highlighting the importance of awareness and early medical evaluation. 2. Why are cancer cases increasing globally? Researchers believe lifestyle changes, environmental exposures, obesity, and improved detection methods all contribute to rising cancer cases. 3. Are cancer cases in India increasing? Yes, healthcare data suggests a steady rise in cancer cases in India, with more diagnoses being reported each year. 4. Why are breast cancer cases in India rising? Factors such as lifestyle changes, hormonal influences, delayed pregnancies, and genetic predisposition may
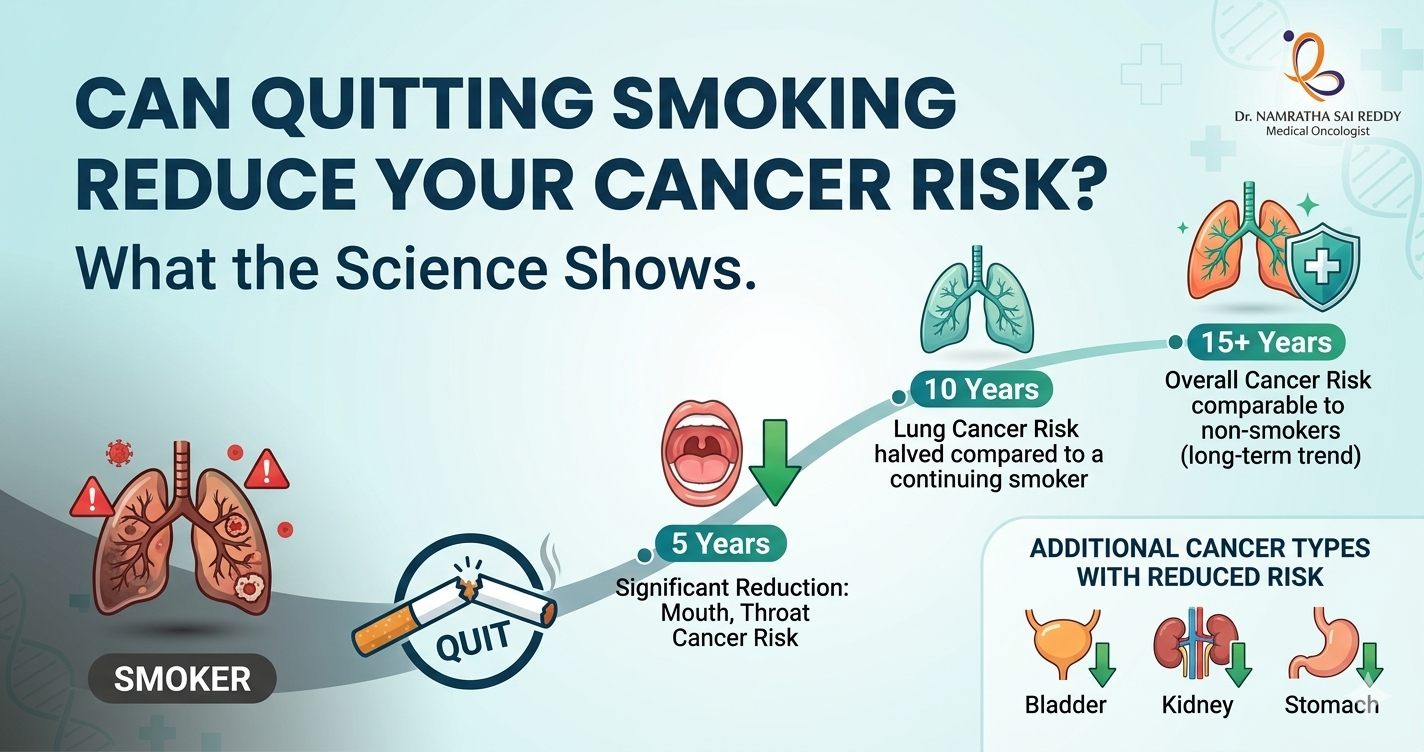
Can Quitting Smoking Reduce Your Cancer Risk? What the Science Shows
Yes, quitting smoking significantly reduces cancer risk at any age. People who quit completely have a 17% lower overall cancer risk than those who continue smoking. Lung cancer risk alone drops by up to 57% for those who quit before age 50, and by 39% for those who quit after 50. Benefits begin within months and compound the longer you stay smoke-free. Key Takeaways Smoking remains one of the leading causes of preventable cancer worldwide. While the dangers of tobacco are well known, many smokers believe that once the damage is done, quitting may not make much difference. Research shows the opposite: quitting smoking at any age significantly reduces cancer risk. The body begins to recover sooner than many people expect, and the most dramatic improvements appear in lung cancer risk. The Link Between Smoking and Cancer Smoking exposes every cell in your body to a barrage of harmful chemicals. According to the American Cancer Society, tobacco smoke contains more than 7,000 chemicals, including at least 70 known carcinogens. These compounds damage DNA, trigger chronic inflammation, and impair the body’s natural ability to repair cells. Tobacco use is strongly associated with multiple cancers, including: • Lung cancer • Liver cancer • Colorectal cancer • Stomach cancer • Bladder cancer • Pancreatic cancer What Research Says About Quitting Smoking A landmark study published in JAMA Network Open analysed health data from nearly 3 million adults over age 30, with an average follow-up period of 13 years. Researchers found that people who quit smoking completely had a 17% lower overall cancer risk compared with those who continued to smoke. The risk reduction varied across different types of cancer: • 42% lower risk of lung cancer • 27% lower risk of liver cancer • 20% lower risk of colorectal cancer • 14% lower risk of stomach cancer Among these, lung cancer risk showed the fastest decline after quitting. Lung Cancer Risk Drops Faster Than Many Expect A long-term analysis from the Framingham Heart Study examined nearly 9,000 participants over a period of 25 to 34 years. The study revealed several important findings: • Nearly 93% of lung cancer cases occurred in heavy smokers. • Within five years of quitting, the risk of lung cancer dropped by about 39% compared with current smokers. • The risk continued to decline the longer someone remained smoke-free. A complementary 2024 study in the Journal of the National Cancer Institute, which tracked over 24,600 Finnish male smokers from 1985 to 2012, confirmed that even simply reducing cigarettes per day lowers lung cancer risk, though completely quitting remains the most effective strategy. However, researchers at CA: A Cancer Journal for Clinicians note that even decades after quitting, former heavy smokers (20+ pack-years) may retain a meaningfully elevated lung cancer risk compared with lifelong non-smokers, underscoring the importance of continued screening. Does Age Matter When You Quit? While quitting at any age offers real benefits, the earlier you stop, the greater the protection. Research reported by Medical News Today and drawn from the JAMA Network Open study shows: The message is clear: it is never too late to quit. Every smoke-free year translates into a measurable reduction in cancer risk. Why Cancer Risk May Appear Higher Shortly After Quitting Some studies have observed a temporary increase in cancer diagnoses within the first few years after quitting. This can seem confusing, but researchers believe it is largely due to what is known as the “sick quitter effect”. In some cases, individuals stop smoking because they are already experiencing early symptoms of illness. As a result, diagnoses may occur shortly after quitting, making it appear as though risk has increased. When researchers account for this factor, the overall trend shows a steady decline in cancer risk following smoking cessation. Health Improvements Begin Quickly After Quitting The body begins repairing itself almost immediately. Here is what research, including findings summarised by the American Cancer Society, shows about the recovery trajectory: Heart rate begins to return to normal levels. Carbon monoxide levels in the blood drop significantly, improving oxygen delivery to cells. Lung function and circulation improve noticeably. Respiratory symptoms like coughing and shortness of breath diminish. Lung cancer risk drops by approximately 39% compared with current smokers (Framingham Heart Study). The risk of several other cancers also begins to fall. Overall cancer risk approaches, though may not fully equal that of lifelong non-smokers, particularly for heavy former smokers. Screening Remains Important for Former Smokers A systematic review published in CA: A Cancer Journal for Clinicians (2023) found that lung cancer risk may remain meaningfully elevated for two to three decades in former heavy smokers, even beyond the 15-year cut-off that currently defines US screening eligibility. The authors argue that age-based screening criteria may be more appropriate than time-since-quitting criteria. Current US Preventive Services Task Force guidelines recommend annual low-dose CT lung cancer screening for adults aged 50 to 80 who have a 20-pack-year smoking history and currently smoke or have quit within the past 15 years. Former heavy smokers should speak with their doctor about continued eligibility. It Is Never Too Late to Quit The evidence is clear. Quitting smoking dramatically reduces cancer risk, and the benefits begin much sooner than most people realise. Even for long-term smokers, stopping today can lead to measurable health improvements within just a few years. While former smokers may still benefit from cancer screening and medical follow-up, the long-term advantages of quitting far outweigh the risks of continuing. Every smoke-free year helps your body heal and lowers your chances of developing cancer. FAQs How soon does cancer risk drop after quitting?Cancer risk begins to decline within a few years, with lung cancer risk dropping significantly within about five years. Is it worth quitting after age 50?Yes. Quitting
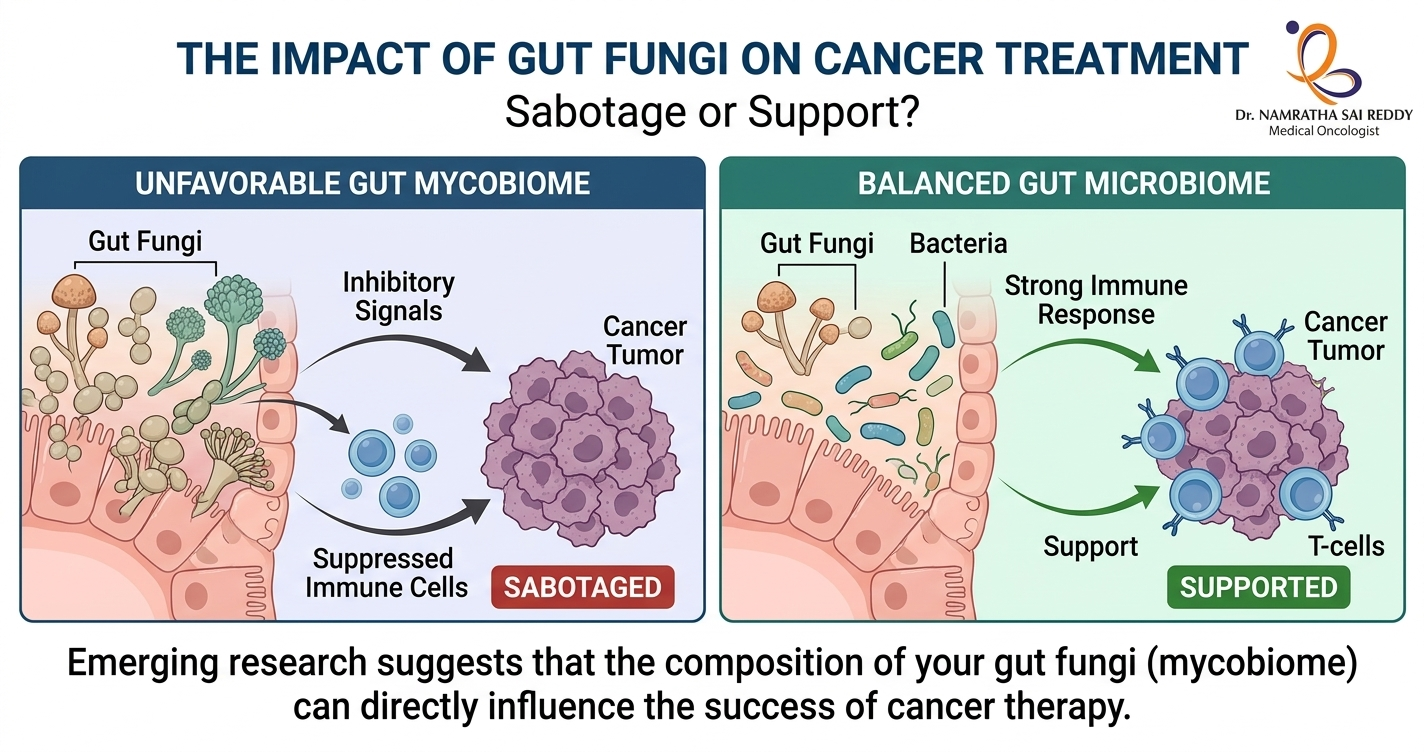
Can Gut Fungi Affect Your Cancer Treatment? What the Science Says
Yes, gut fungi can affect cancer treatment outcomes. Research published in Cancer Cell by scientists at Cedars-Sinai Medical Centre found that intestinal fungi suppress anti-tumour immune responses after radiation therapy. Fungal overgrowth, which frequently follows antibiotic use, was shown to reduce treatment effectiveness in models of both breast cancer and melanoma. Treating the animals with antifungal drugs restored the immune response and improved outcomes. Scientists now believe the gut mycobiome may be one of the missing pieces explaining why only 20 to 40% of patients respond to immunotherapy. Key Takeaways What Is the Gut Mycobiome? The human gut hosts approximately 38 trillion microorganisms, including bacteria, fungi, viruses, and other microbes. While research has traditionally focused on bacteria, the gut’s fungal community (the mycobiome) is now attracting serious scientific attention. Fungi make up just 0.01 to 2% of cells in the gut microbiome, but researchers have reliably identified 50 to 100 fungal genera living there. These fungi colonise early in life through birth, breastfeeding, food intake, and environmental exposure. Under normal conditions, they are non-pathogenic. However, when bacterial populations decline or the immune system is disrupted, fungal communities can shift dramatically, with serious downstream effects on immunity and treatment response. The Cedars-Sinai Study: Fungi and Radiation Therapy The most significant study in this field to date was led by Dr. Stephen Shiao and Dr. David Underhill at Cedars-Sinai Medical Centre. Published in Cancer Cell, the research found that intestinal bacteria and fungi have directly opposing effects on anti-tumour immune responses following radiation therapy. Consistent results were observed across both breast cancer and melanoma models, suggesting the findings may apply broadly across cancer types. Key findings: This is clinically relevant because antibiotics are routinely prescribed to cancer patients who are at elevated infection risk. The study suggests that this common practice may, in some cases, inadvertently compromise treatment outcomes by promoting fungal overgrowth. The Dectin-1 Connection: How Tumours Sense Fungi A key discovery from the Cedars-Sinai research was the role of a fungal-sensing immune receptor called Dectin-1. This protein detects beta-1,3-glucan, a compound in fungal cell walls, and activates the body’s antifungal immune pathways. It is primarily expressed in macrophages and dendritic cells within tumours. Using data from The Cancer Genome Atlas, the researchers found: As the National Cancer Institute noted in its coverage of the study, Dectin-1 could serve as a biomarker to identify patients with an unfavourable microbiome composition ahead of treatment. Specific Fungi Linked to Cancer Risk A comprehensive review published in Gut Microbes (2025) highlights specific fungal species now linked to distinct cancer outcomes: The review also notes that in cancer patients, the gut mycobiome undergoes substantial remodelling in both its composition and ecological structure. These shifts are increasingly recognised as important modulators of disease progression, immune dynamics, and responsiveness to therapy. How Gut Fungi Influence Immunotherapy Immunotherapy works by activating immune cells to recognise and destroy cancer. Research published in npj Biofilms and Microbiomes (2025) outlines the key mechanisms through which gut fungi influence this process. Immune signalling modulation – Fungal molecules interact with immune receptors such as Dectin-1 and can shift the immune environment towards tolerance and suppression rather than active tumour-fighting. Tumour microenvironment changes – According to a 2026 review in Gut Microbes, fungi and their metabolites remodel the tumour microenvironment through metabolic reprogramming, including depletion of critical amino acids and production of immunosuppressive short-chain fatty acids. Microbial balance disruption – When bacterial diversity drops following antibiotic use, poor diet, or illness, fungi overgrow and disrupt the anti-tumour immune activity that bacteria normally support. This balance is now considered a critical regulator of cancer treatment response. Impaired CD8 T cell activity – The Cedars-Sinai study found that fungal overgrowth impairs the activity of cytotoxic CD8 T cells (the immune cells most critical for killing cancer cells) while increasing immunosuppressive macrophages in the tumour microenvironment. A Fast-Moving Field: Research Milestones The relationship between the gut microbiome and immunotherapy is one of oncology’s fastest-growing research areas. Research published in iMeta (2024) documents the following milestones: A landmark review in Nature Reviews Drug Discovery (2025) concludes that the gut microbiome is now recognised as a key modulator of immunotherapy efficacy, with clinical trials of microbiome-based interventions actively underway. The Future of Microbiome-Driven Cancer Care Researchers highlighted in a Nature collection on the microbiome in cancer (2024) note that tumours contain both bacteria and fungi, and that their presence is proving useful in detecting cancers, categorising them, and predicting whether specific interventions will work. Potential future strategies include: A 2026 review in Gut Microbes concludes that fungi and their metabolites may enhance tumour immunogenicity and reduce therapeutic resistance, with antifungal-based therapies showing particular promise as an adjunct to immunotherapy. What This Means for Cancer Patients Cancer therapy is no longer just about targeting tumour cells. The microbial ecosystem inside the body plays a significant role in determining treatment success. As Dr. David Underhill of Cedars-Sinai stated after the landmark study: “It would be really handy to be able to characterise a patient’s microbiome, both bacterial and fungal, and determine their expected prognosis, or how they will respond to radiation therapy, chemotherapy, or immunotherapy. Then we would like to see whether it is feasible to change that microbiome to make those therapies work better.” The gut microbiome, including its fungal residents, may soon become one of oncology’s most important biomarkers and therapeutic targets. FAQs Can gut fungi actually affect cancer treatment outcomes? Yes. Research in Cancer Cell shows that gut fungi directly suppress anti-tumour immune responses after radiation therapy. Antifungal treatment restored immune activity and improved outcomes in preclinical models of breast cancer and melanoma. Why do some patients not respond to immunotherapy? Multiple factors contribute, including tumour genetics, immune profile, and gut microbiome composition. Only 20 to 40% of patients in certain groups respond to immunotherapy. Scientists believe optimising the mycobiome may help improve these rates. What is Dectin-1, and why does it matter in cancer? Dectin-1 is an immune receptor that senses fungi. Higher Dectin-1 expression in
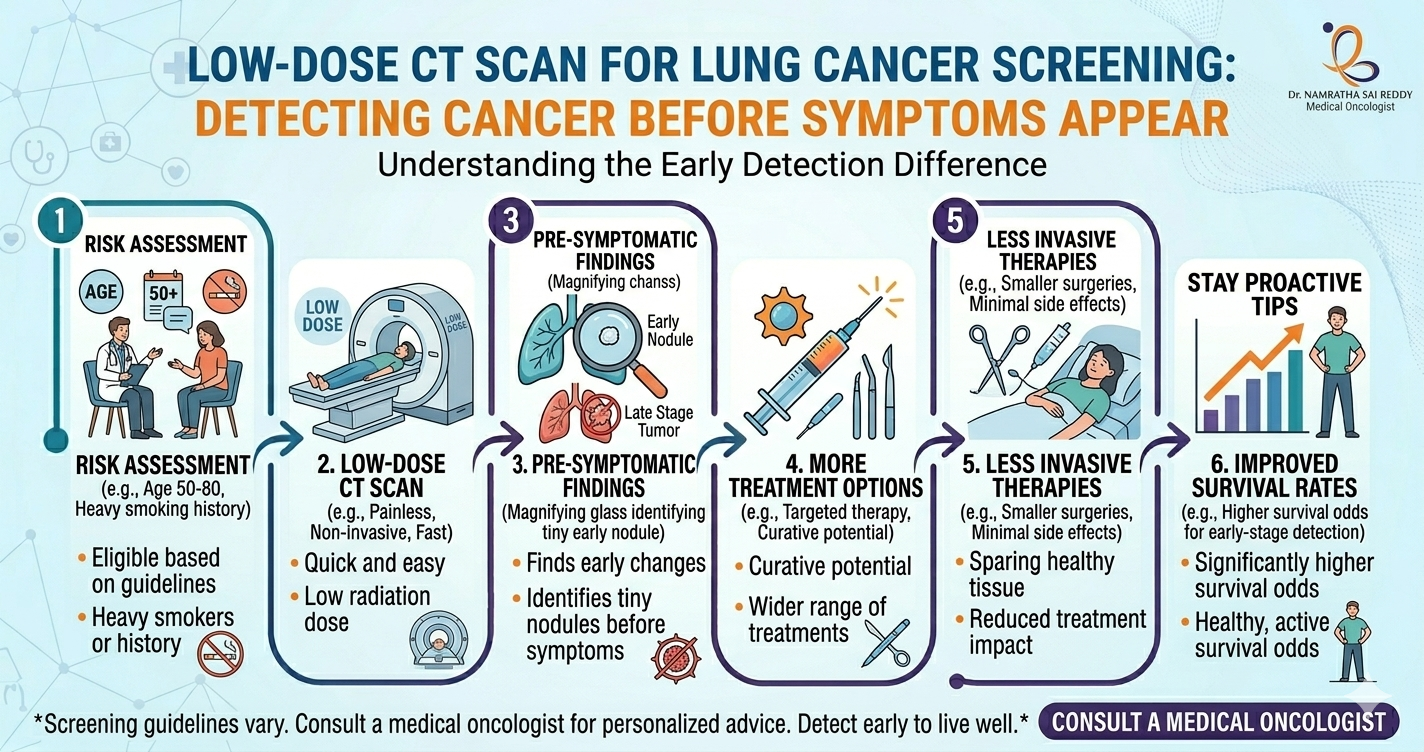
Low-Dose CT Scan for Lung Cancer Screening: Detecting Cancer Before Symptoms Appear
Lung cancer remains one of the most serious global health challenges. One major reason is that the disease often develops without noticeable symptoms in its early stages, leading to delayed diagnosis and limited treatment options. Advances in medical imaging have changed this reality. One of the most important breakthroughs in cancer screening is the Low-Dose CT (LDCT) scan, which allows doctors to detect lung cancer much earlier than traditional methods. Research has shown that screening high-risk individuals with LDCT can reduce lung-cancer deaths by about 20% compared with chest X-rays, demonstrating the powerful role of early detection in saving lives. Key Takeaways What Is a Low-Dose CT Scan for Lung Cancer Screening? A low-dose CT scan is a specialised imaging test designed to detect lung cancer in people who are at higher risk of developing the disease. Unlike a standard CT scan, LDCT uses significantly less radiation while still producing detailed images of the lungs. This enables doctors to detect very small nodules or abnormalities that may indicate early cancer, often before symptoms appear. How the technology works Low-dose CT scans use advanced imaging technology to capture multiple cross-sectional images of the lungs from different angles. A computer then processes these images to create a detailed view of lung tissue. This level of precision allows doctors to detect nodules as small as a few millimetres in size, which would typically not be visible on a standard chest X-ray. Key features of LDCT screening Because lung cancer often progresses silently, this technology has become one of the most valuable tools in early cancer detection. Why Is Early Detection of Lung Cancer So Important? Early detection dramatically improves survival rates. Lung cancer often does not cause noticeable symptoms until the disease has progressed. When symptoms such as persistent cough, chest pain, fatigue, or weight loss appear, the cancer may already have spread. Detecting lung cancer earlier can significantly improve treatment outcomes. Statistics highlighting the importance of early detection Benefits of detecting cancer early Early diagnosis may allow doctors to: For many patients, early detection can mean the difference between curative treatment and complex long-term management. Who Should Consider Low-Dose CT Screening? Adults at high risk, especially long-term smokers. Not everyone requires lung cancer screening. The benefits of LDCT screening are greatest in individuals with higher risk factors, particularly long-term smokers. Recommended screening group Medical guidelines generally recommend screening for individuals who: Understanding pack-years A pack-year is a measurement used to estimate long-term smoking exposure. Examples include: Both scenarios equal 20 pack-years of smoking exposure. Other potential risk factors Some individuals may also have an elevated risk due to: A healthcare provider can help determine whether screening is appropriate based on individual risk factors. What Happens During a Low-Dose CT Scan? A fast, painless imaging test of the lungs. Many patients feel anxious before undergoing imaging tests. However, the low-dose CT scan is simple, quick, and painless. Step-by-step overview The entire process usually takes less than 10 minutes, and no recovery time is needed. Important features of the procedure Because of its simplicity and low radiation exposure, LDCT is considered safe for annual screening in eligible individuals. What Can a Low-Dose CT Scan Detect? Tiny nodules and early signs of lung cancer. One of the biggest advantages of LDCT scans is their ability to detect very small lung abnormalities that may not appear on standard imaging tests. Possible findings on the scan It is important to understand that most lung nodules detected during screening are not cancerous. What happens if a nodule is detected? If an abnormality appears on the scan, doctors may recommend: Careful monitoring helps determine whether a nodule is harmless or requires further evaluation. What Are the Benefits of Low-Dose CT Screening? Low-dose CT screening offers several important advantages, especially for individuals at higher risk. Major benefits include Early cancer detection The scan can detect tumours before symptoms develop, improving treatment success. Improved survival rates Early-stage lung cancer is often more treatable and may be cured through surgery. Non-invasive procedure The screening test is quick, painless, and does not require hospitalisation. Better monitoring of lung health The scan may also detect other lung conditions that require medical attention. Are There Any Risks or Limitations? While LDCT screening provides many benefits, it is important to understand potential limitations. False positives Sometimes scans may detect nodules that appear suspicious but are not cancerous. This may require additional testing. Radiation exposure Although the radiation dose in LDCT scans is significantly lower than that of standard CT scans, repeated imaging over time may increase cumulative exposure. Overdiagnosis In rare cases, screening may detect very slow-growing cancers that might not have caused symptoms during a person’s lifetime. Because of these factors, screening is recommended primarily for individuals who meet established risk criteria. How Can People Reduce Their Risk of Lung Cancer? While screening helps detect cancer early, prevention remains the most effective strategy. Avoid smoking and maintain healthy habits. Steps that reduce lung cancer risk Combining preventive measures with appropriate screening provides the best protection against lung cancer. Prioritize Prevention and Early Detection for Better Lung Health Low-dose CT scans represent a major advancement in the early detection of lung cancer. By identifying abnormalities before symptoms appear, this screening method allows doctors to intervene earlier and improve treatment outcomes. For individuals with a significant smoking history or other risk factors, discussing low-dose CT screening with a healthcare professional may be an important step toward protecting long-term health. Early detection not only improves survival rates but also offers patients a better chance at effective treatment and recovery. Frequently Asked Questions (FAQs) 1. What is a low-dose CT scan? A low-dose CT scan is an imaging test that uses minimal radiation to detect early lung abnormalities that may indicate cancer. 2. Who should undergo lung cancer screening? Adults aged 50–80 with a significant smoking history or those who quit smoking within the past 15 years are typically recommended for screening. 3. Is the low-dose CT scan
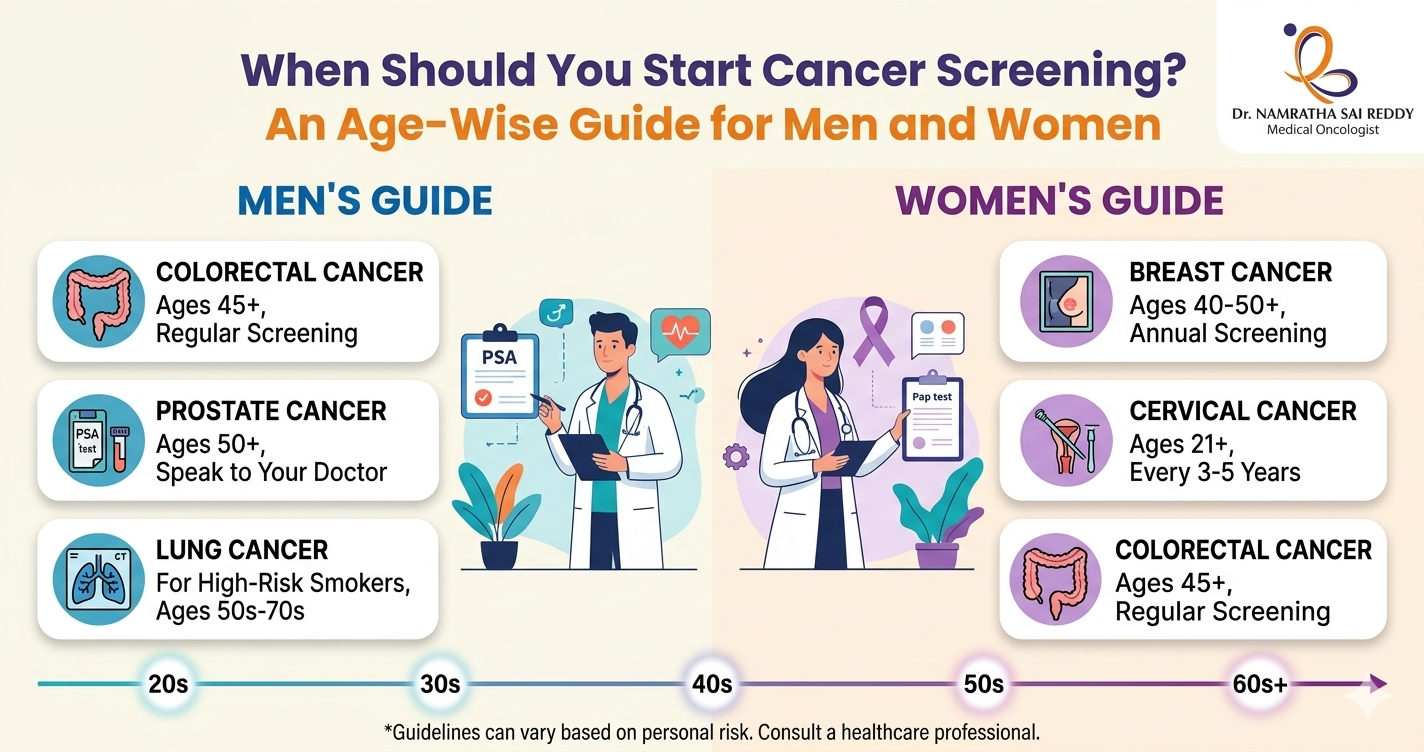
When Should You Start Cancer Screening? An Age-Wise Guide for Men and Women
• Most cancer screenings begin between the ages of 21 and 50. Missing or delaying them is one of the biggest reasons cancers go undetected until they’re harder to treat. • Women start cervical screening at 21, mammograms at 40; everyone starts colorectal screening at 45; men discuss prostate screening at 50. Knowing your age-based schedule removes the guesswork. • Pap smears and colonoscopies can catch and remove precancerous cells before they turn malignant, making them true prevention tools. • Family history, genetic mutations (BRCA, Lynch syndrome), smoking, or prior precancerous conditions can move your screening start date earlier. Talk to your doctor if any of these apply. • Regular screening, even when you feel completely fine, is what makes early detection possible. Cancer screening should begin at age 21 for women (cervical cancer) and age 45 for both men and women (colorectal cancer). Women should start mammograms at 40, and men should discuss prostate screening at 50. The right age depends on cancer type, gender, and personal risk factors. Cancer often develops silently, without obvious symptoms in its early stages. That is why screening plays a crucial role in preventive healthcare. Cancer screening tests help detect abnormal cells or early-stage cancers before symptoms appear, allowing treatment to begin when it is most effective. Why Cancer Screening Is Important Cancer screening helps detect disease before symptoms appear. Early detection significantly improves treatment outcomes and survival rates. Most early-stage cancers have survival rates of 80 to 90 percent, while advanced-stage cancers are far more difficult to treat. According to the AACR Cancer Progress Report 2024, overall cancer death rates in the United States fell by 33 percent between 1991 and 2021, translating to an estimated 4.1 million lives saved, a trend driven in large part by earlier detection through screening. Screening also identifies precancerous changes, allowing doctors to treat them before cancer develops. For example, colonoscopies and Pap tests can prevent certain cancers entirely, not just detect them early. Key benefits of cancer screening include: • Early diagnosis and timely treatment • Improved survival rates • Less aggressive treatment options • Better quality of life • Prevention of certain cancers Ages 21 to 29: Early Preventive Screening In this age group, routine screening begins primarily for women. For Women Cervical Cancer Screening Women should begin Pap smear screening at age 21, regardless of sexual activity. The recommended schedule is a Pap test every three years between the ages of 21 and 29. Pap tests detect abnormal cervical cells that may eventually develop into cervical cancer. Breast Awareness Women should begin monthly breast self-examinations from age 20 and consult a doctor if they notice lumps, breast pain, or changes in breast shape or skin. For Men Routine cancer screening is not typically recommended for most men in this age group unless there are specific risk factors. Men should still attend regular health check-ups that include general examinations for skin changes, lumps or swelling, and abnormal growths. Men with a strong family history of cancer may require earlier screening discussions with their doctor. Ages 30 to 39: Expanding Screening In your thirties, screening continues for cervical cancer and preventive health evaluations. For Women Cervical Cancer Women aged 30 to 65 should undergo either a Pap smear plus HPV test every five years, or a Pap smear alone every three years. HPV testing helps detect high-risk strains of human papillomavirus, which are responsible for approximately 99 percent of all cervical cancers. Breast Cancer Routine mammograms are not yet recommended for average-risk women in their thirties. Those with a family history, BRCA gene mutation, or other elevated risk factors should discuss earlier screening with their doctor. For Men Routine screening is still limited at this age. Men should monitor their health and consult a doctor if they notice persistent fatigue, unexplained weight loss, or lumps and unusual swelling. Men with genetic or family cancer risk may require earlier screening discussions. Ages 40 to 49: An Important Screening Stage Cancer screening becomes more structured during this decade. For Women Breast Cancer Women should begin annual mammograms starting at age 40. Mammography can detect breast cancer before symptoms appear, significantly improving survival rates. Thanks in part to early mammography, most breast cancers today are diagnosed at stage I, which carries a five-year survival rate of close to 100 percent. Cervical Cancer Continue screening with a Pap plus HPV test every five years, or a Pap test alone every three years. For Men (High Risk) Prostate Cancer Men with increased risk, such as a family history of prostate cancer or of African American descent, should discuss screening with their doctor starting at age 45. Screening may include a PSA (prostate-specific antigen) blood test and a digital rectal examination (DRE). For Both Men and Women Colorectal Cancer Routine screening for colorectal cancer should begin at age 45 for most adults. Thanks to screening, colorectal cancer death rates have fallen by 47 percent in men and 44 percent in women over recent decades. Ages 50 to 64: Comprehensive Cancer Screening In your fifties and early sixties, screening becomes essential across multiple cancer types. For Women Women should continue annual mammograms. Cervical cancer screening continues with a Pap plus HPV test every five years, or a Pap smear every three years. For Men Prostate Cancer Men aged 50 and above should discuss prostate cancer screening with their doctor. Testing may include a PSA blood test and a digital rectal exam. Shared decision-making, weighing the potential benefits and harms of screening is recommended. For Both Men and Women Colorectal Cancer Recommended screening methods include a colonoscopy every ten years, annual stool tests (FIT or FOBT), flexible sigmoidoscopy every five years, or a stool DNA test every three years. Colonoscopy remains the gold standard because it can both detect and remove precancerous polyps during the same procedure. Lung Cancer Adults aged 50 to 80 with a heavy smoking history like 20 pack-years
Can the HPV Vaccine Prevent Cervical Cancer? Here’s the Science
Yes, and the evidence is overwhelming. HPV vaccination reduces cervical cancer risk by up to 88–90% when given before age 17. In India, where a woman dies of cervical cancer every seven minutes, the HPV vaccine is not just a health tool; it is a national emergency intervention. India launched its nationwide free vaccination programme on 28 February 2025, targeting 11.5 million girls aged 14. Key Takeaways • India carries the world’s highest cervical cancer death toll. Over 79,906 women died from cervical cancer in India in 2022, more than 22% of all global deaths and a new case is diagnosed every four minutes. • HPV causes virtually all cervical cancers in India. HPV types 16 and 18 alone account for 76.7% of cervical cancer cases in India, making targeted vaccination extraordinarily effective. • Early vaccination delivers the strongest protection. Girls vaccinated before age 14 need only 2 doses and gain up to 90% risk reduction. Waiting until adulthood significantly reduces the vaccine’s benefit. • India now has an affordable home-grown vaccine. CERVAVAC by the Serum Institute of India costs ₹1,400–2,500 per dose in private clinics — and is free at government centres for eligible girls under the national programme. • Vaccination and screening must go together. The HPV vaccine does not protect against all high-risk strains. Regular Pap smears or HPV DNA tests remain essential, yet India’s current cervical cancer screening rate is just 2%. The Link Between HPV and Cervical Cancer Human Papillomavirus (HPV) is the most common sexually transmitted infection worldwide. While most HPV infections clear on their own, certain high-risk strains can persist and cause cancers of the cervix, vagina, vulva, penis, anus, and throat. Cervical cancer is the most common HPV-related cancer in women. According to the WHO’s Global Strategy for Cervical Cancer Elimination (2025), approximately 660,000 new cases and 350,000 deaths occurred in 2022 alone, with the highest burden in low- and middle-income countries. In India, cervical cancer claims one woman’s life every eight minutes and accounts for approximately 1.23 lakh new cases per year. Approximately 99.7% of all cervical cancers are caused by untreated or chronic HPV infection, making it one of the most preventable of all cancers. HPV types 16 and 18 alone are responsible for around 70% of all cervical cancer cases globally. How the HPV Vaccine Prevents Cervical Cancer The HPV vaccine is a preventive injection, not a treatment. It works by training your immune system to recognise specific high-risk HPV strains before exposure. When a vaccinated person later encounters the virus, their immune system neutralises it before it can establish a persistent infection that leads to cancer. Think of it as the only shot specifically designed to prevent cancer. The HPV vaccine is not just a vaccine against a virus; it is a vaccine against cancer. The “shot to prevent cervical cancer” and the “injection to prevent cervical cancer” both refer to the HPV vaccine, available in India as Gardasil, Gardasil 9, Cervarix, and CERVAVAC. It is administered as an intramuscular injection into the upper arm. HPV Vaccine Types Available in India As of 2025, India has four approved HPV vaccines. Each differs in the number of HPV strains covered, the approved age range, and cost. Gardasil 9 (Nonavalent) • Strains covered: HPV 6, 11, 16, 18, 31, 33, 45, 52, 58 (9 strains) • Age range: 9–45 years • Broadest available protection against HPV-related cancers and genital warts Gardasil 4 (Quadrivalent) • Strains covered: HPV 6, 11, 16, 18 • Age range: 9–26 years • Also prevents genital warts Cervarix (Bivalent) • Strains covered: HPV 16, 18 • Age range: 9–25 years • Targets the two main cancer-causing HPV strains CERVAVAC (Made in India – Bivalent) • Strains covered: HPV 16, 18 • Age range: 9–26 years • Developed by the Serum Institute of India, the most affordable option available • Launched in 2023 as India’s first indigenously developed HPV vaccine HPV Vaccine Dosing Schedule: 2-Dose vs 3-Dose The number of doses you need depends on your age when you receive your first shot. The younger you are when you are vaccinated, the stronger your immune response and the fewer doses you will need. 2-Dose Schedule (Ages 9–14) Children in this age group require only two doses because their immune response is stronger. 3-Dose Schedule (Ages 15 and Older) The CDC recommends routine vaccination at ages 11 or 12 (beginning as early as age 9), well before potential exposure to HPV. Immunocompromised individuals aged 9–26 require three doses regardless of their age at first vaccination. Note on single-dose schedules: As of early 2026, 89 countries, including the United States, have adopted a single-dose schedule for national immunisation programmes, particularly for Gavi-eligible low-income countries. Multi-dose schedules remain standard in India’s private market. Why Is the HPV Vaccine Not Recommended After Age 26? This is one of the most common questions about the HPV vaccine. The answer lies in biology and health economics. The CDC’s Advisory Committee on Immunisation Practices (ACIP) does not recommend routine HPV vaccination for adults over 26 for the following reasons: 1. Prior Exposure Reduces Benefit Most sexually active adults have already been exposed to one or more HPV strains by their mid-20s. Since the vaccine prevents infection but cannot treat existing HPV, its protective benefit is significantly lower in this age group. 2. Limited Cost-Effectiveness at the Population Level A landmark study by Harvard T.H. Chan School of Public Health, published in PLOS Medicine, found that vaccinating adults beyond age 26 provides limited health benefit at the population level at a substantial cost. The study modelled HPV-associated cancer and genital wart outcomes across multiple age-group scenarios. 3. FDA Approval Up